



Informed Immunity: Autism Anonymous (Part 2/3)
Learn about the current vaccination schedule, public concerns, and the facts behind vaccine safety and scheduling.
When you think about vaccines, you probably imagine a little pinch, a Band-Aid, and a sigh of relief knowing you're protected.
But have you ever wondered what’s inside that tiny vial?
Among the many ingredients, there’s one name that comes up more than any other: Thiomersal (or Thimerosal, as it's called in the U.S.). This mercury-based preservative has been the center of heated debates for decades, with some hailing it as a necessary safeguard for public health and others calling it a toxic threat.
But what does the data say?
Thiomersal’s story is anything but straightforward. It’s been used in vaccines since the 1930s, quietly doing its job of preventing contamination. Yet, its role became much more controversial during a critical period between 1989 and 1993, when vaccine schedules expanded rapidly, and Thiomersal found its way into more and more doses.
So, why is Thiomersal in vaccines in the first place?
Is it the unsung hero that keeps vaccines safe from harmful bacteria, or is it contributing to long-term health risks?
Or even death?
History of Thiomersal in Vaccines


Vaccines were becoming a game-changer in the 1920s. This is the age of tuberculosis, diphtheria, smallpox, and the like.
However, it faced a significant problem: contamination. Multi-dose vaccine vials—used to immunize large groups efficiently—were vulnerable to bacterial and fungal growth after being opened. And it was bad. In Columbia, South Carolina, in 1916, a tainted batch of typhoid vaccine stored at room temperature caused 68 severe reactions, 26 abscesses, and 4 deaths.
Enter Thiomersal. In 1928, researchers at Eli Lilly and Company discovered Thiomersal (known as Thimerosal in the U.S.), a compound containing ethylmercury. It acted as a preservative that killed or inhibited the growth of bacteria and fungi.
It was launched in 1930 and was put into their vaccines. Thiomersal was a mercury-based antiseptic and germicide that "had been formulated at the University of Maryland with support of a Lilly research fellowship."
Was Thiomersal Always Bad?
History of Concern: Merthiolate
Thiomersal (also known as Merthiolate) was first introduced in 1928 by Eli Lilly and Company as a mercury-based preservative intended to prevent bacterial and fungal contamination in multi-dose vaccine vials. It was hailed as a breakthrough in vaccine preservation, especially during an era when contamination posed significant risks to public health. Thiomersal was quickly adopted for use in vaccines such as the diphtheria toxoid and tetanus vaccines, where it played a key role in ensuring safety during storage and transportation.
However, by the 1930s, early safety concerns began to emerge. A 1935 letter to Eli Lilly highlighted that animal studies, including tests on dogs, showed adverse reactions to Thiomersal. Researchers reported symptoms consistent with mercury poisoning, such as tremors and neurological impairments, raising questions about its safety. Despite these findings, no regulatory changes were made, and Thiomersal continued to be used widely.
By the 1940s, additional reports surfaced documenting toxic effects in both animals and humans exposed to Thimerosal. For example, a 1948 study published by the American Medical Association (AMA) Blue Ribbon Committee noted that mercury levels in Thimerosal were dangerously high, with toxicity thresholds comparable to other known hazardous substances.
Despite these red flags, Thiomersal’s practicality and low cost made it indispensable for vaccine manufacturers, who relied on multi-dose vials to reduce production and distribution expenses.
AKA: The profit was too good to pass up.
Over the following decades, the use of vaccines containing Thiomersal increased significantly.
What Makes It Bad?
Ethyl vs. Methyl Mercury
One of the main debates revolves around ethyl mercury (found in Thiomersal) versus methyl mercury (found in fish and environmental sources). The latter has had a plethora of research in support of watching the amount of fish you eat specifically because of the mercury levels.
While both are forms of mercury, their toxicity and behavior in the body differ:
Ethyl Mercury:
Found in vaccines.
Processes faster in the body than methyl mercury but converts to inorganic mercury in the brain.
A 2015 study shows that ethyl mercury is 50x more toxic to human cells than methyl mercury.
Methyl Mercury:
Found in seafood.
Stays in the bloodstream longer, but its neurological effects are well-documented.
Mercury Levels Comparison - What is Inorganic Mercury and Is It Toxic?
When ethyl mercury—the type of mercury found in Thiomersal—is metabolized by the body, it breaks down into inorganic mercury. This inorganic form tends to accumulate in the brain and is more challenging for the body to eliminate compared to organic forms. Studies have shown that inorganic mercury can disrupt cellular processes and lead to neuroinflammation, impacting neurological function.
In today's world, it's exceedingly rare for someone to have zero mercury exposure. Mercury is a naturally occurring element found in air, water, and soil. Human activities like coal-burning power plants, mining, and certain manufacturing processes release additional mercury into the environment. For example:
Air Pollution: Mercury emitted into the atmosphere can travel long distances before settling into waterways and soil. Breathing air near industrial sites can lead to direct exposure.
An example of this was in Leominster, Massachusetts in relation to the Foster Grant Plant. Approximately 100 children who were born near the plant were autistic.
Unfortunately for the parents, it was determined that, because the children didn’t have any chromosomal irregularities, it wasn’t the plant’s fault…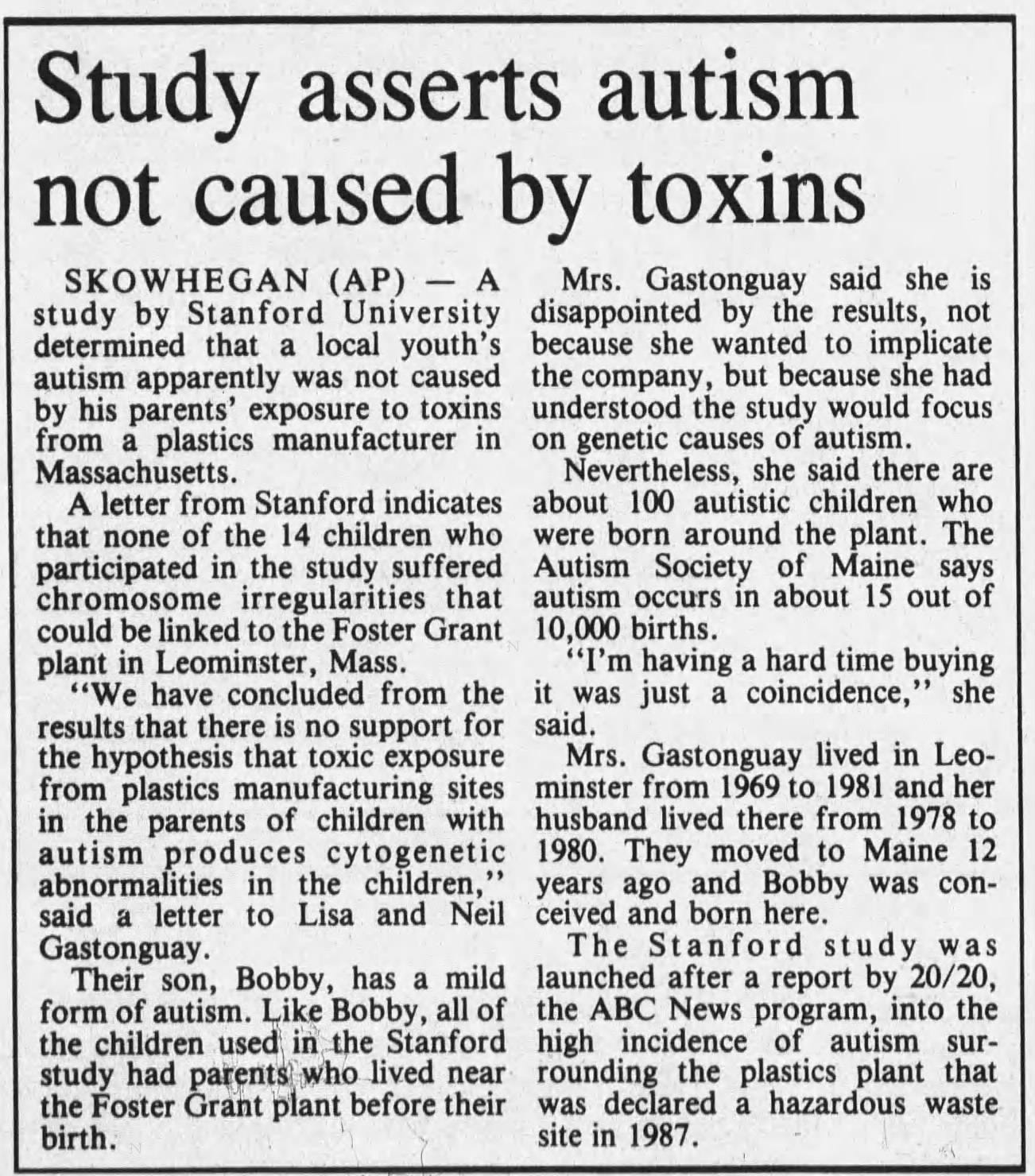
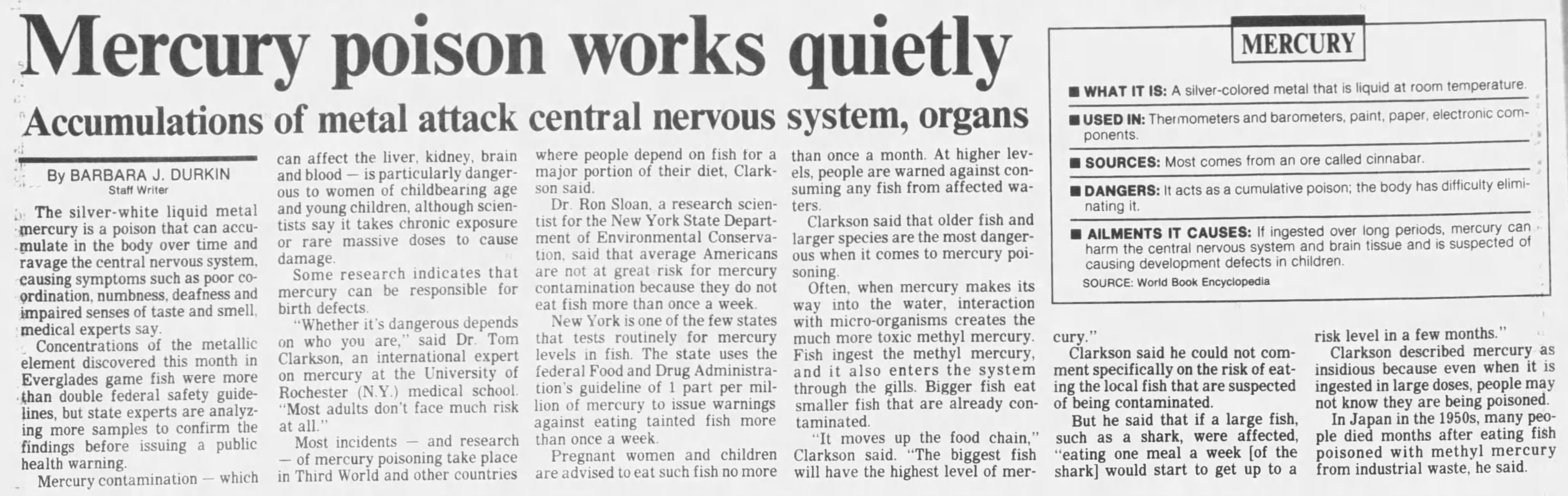
Kennebec Journal. July 7, 1993. Seafood Consumption: Microorganisms in water bodies convert mercury into methyl mercury, which accumulates in fish and shellfish. Eating seafood—especially larger fish like tuna, swordfish, and king mackerel—can result in higher intake of methyl mercury.
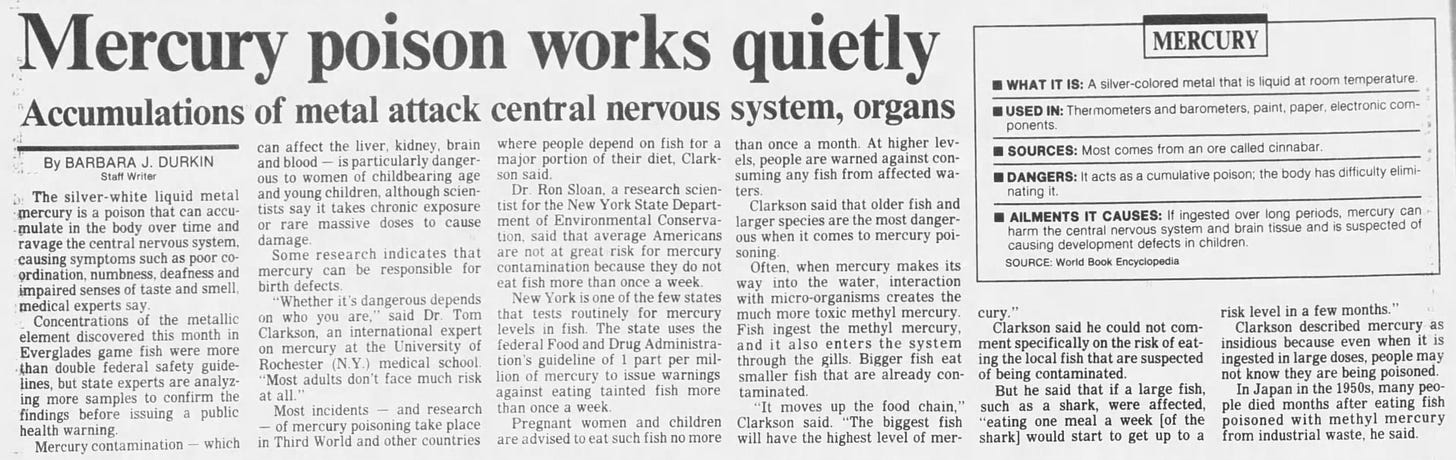
South Florida Sun Sentinel. Feb 22, 1989. Household Products: Items like fluorescent light bulbs, batteries, and some cosmetics contain small amounts of mercury, contributing to everyday exposure.
According to the Environmental Protection Agency (EPA), nearly all people have at least trace amounts of mercury in their bodies due to these environmental sources. While the average dietary exposure to methyl mercury is below levels associated with harm, the cumulative effect is a concern, particularly for pregnant women, infants, and young children whose developing nervous systems are more susceptible to toxins.
Vaccines containing Thiomersal add to this overall mercury burden.
Before Thiomersal was reduced or removed from some childhood vaccines in the early 2000s, infants could receive up to 187.5 micrograms of mercury by six months old from vaccinations alone.
A study published in Environmental Health Perspectives explored how prenatal and early-life exposure to mercury can affect neurodevelopment. The researchers found associations between higher mercury levels and deficits in cognitive functioning.
Another study in the Journal of Neurochemistry highlighted how inorganic mercury in the brain could interfere with neurotransmitter systems, potentially leading to neurological issues.
Given that mercury exposure is virtually unavoidable due to environmental factors, the addition of even small amounts from vaccines containing Thiomersal has amplified concerns. This has led to ongoing debates about the safety of cumulative mercury exposure, especially in infants and young children, and underscores the importance of minimizing unnecessary sources of mercury whenever possible.
How Much Micrograms of Mercury Are Kids Getting?
The amount of mercury children are exposed to has been a source of growing concern, especially during the height of Thiomersal use in vaccines. In the late 1980s and early 1990s, infants following the standard vaccination schedule could receive up to 187.5 micrograms of mercury by the time they were six months old. This total came from multiple doses of vaccines such as Hepatitis B, DTaP, and Hib, all of which contained Thiomersal as a preservative.
Mercury in Vaccines vs. Environmental Standards
To understand the significance of this exposure, let’s compare it to established guidelines for mercury intake from other sources:
The Environmental Protection Agency (EPA) sets the maximum allowable concentration of mercury in drinking water at 2 parts per billion (ppb).
The FDA and EPA recommend that pregnant women, nursing mothers, and young children limit their mercury intake from fish to 0.1 micrograms per kilogram of body weight per day. For a 10-kilogram (22-pound) child, this equals 1 microgram per day.
Standard Flu Shot:
Multi-dose vials of the flu vaccine, which still contain Thiomersal, have about 25 micrograms of mercury per dose in the form of ethyl mercury.
This is 25x higher than the daily limit for mercury intake from fish for a child, as recommended by the EPA. On top of that, this is ethyl mercury which is 50x more harmful.

What’s the Connection to Autism?
Historical Connection
The suspicion of a link between vaccines and autism dates back to anecdotal reports of developmental regression following vaccinations. However, it wasn’t until the 1990s that researchers and parents began associating autism rates with vaccine schedules containing Thiomersal.



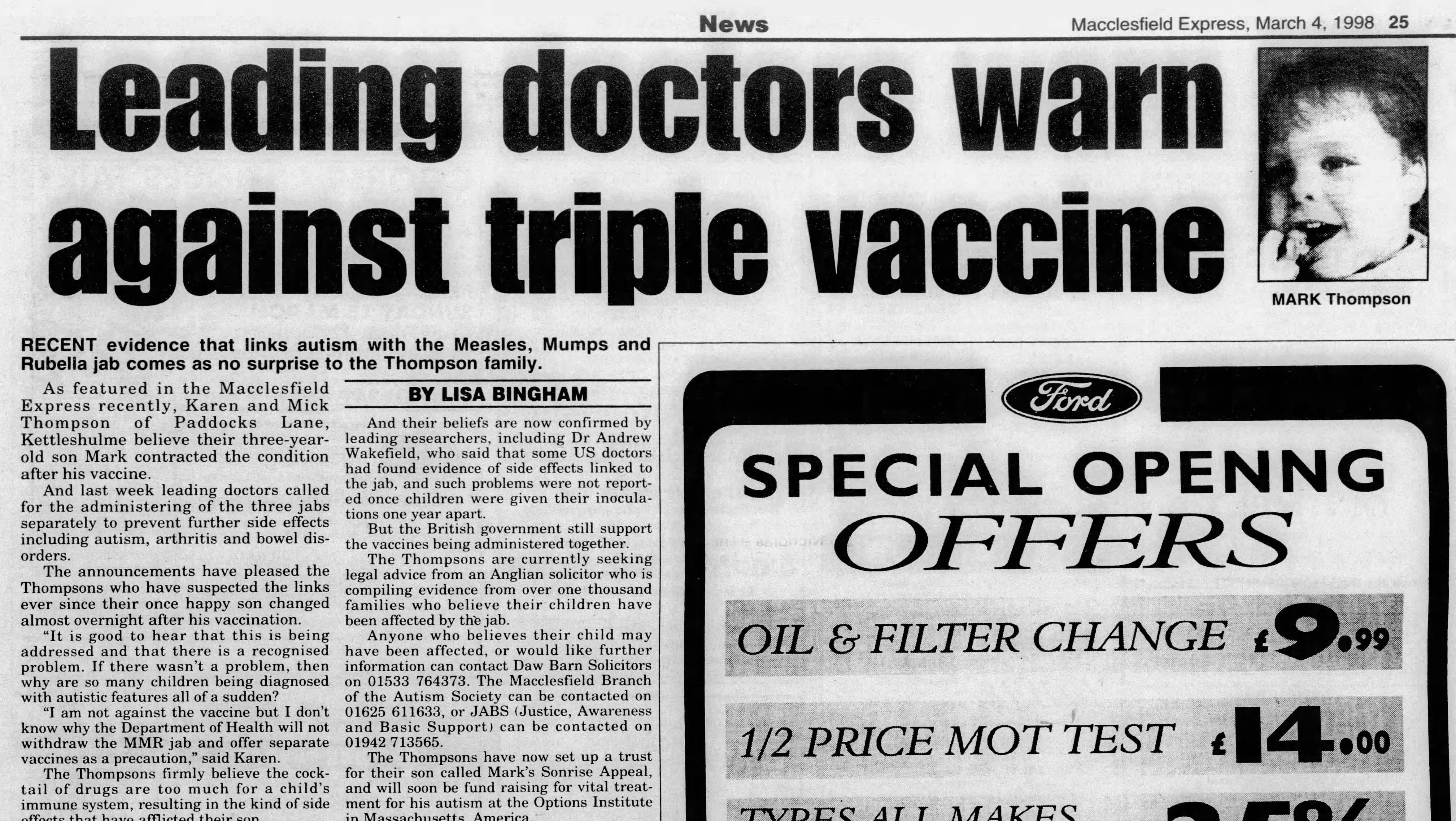
This connection gained public attention when Dr. Andrew Wakefield published a controversial and later “discredited” paper in 1998, linking the MMR vaccine to autism. Dr. Wakefield himself said he never said that there was causation but that the findings warranted further research. He also recommended that the MMR vaccine be given in 3 shots, instead of one.
That was it.
He believed that parents “are the best observers of their children” and that “parents know best.”
Correlation of Autism Rate to Rate of Vaccination
Dr. Wakefield’s concerns weren’t unwarranted. The rise in autism diagnoses coincided with an increase in vaccine recommendations:
1989–1992: Hepatitis B and Hib vaccines were added to the childhood schedule, both of which were administered in multi-dose vials.
Autism rates jumped from 1 in 10,000 in the 1980s to 1 in 500 by the late 1990s.
While improved diagnostics contributed to this rise, some researchers suspeccted the vaccines (or rather cumulative mercury exposure) as a potential factor.

National Childhood Vaccine Injury Act (NCVIA)
Passed in 1986, the NCVIA also contributed to the increase of vaccinations and th use of Thiomersal. The NCVIA (discussed in part 1 of this series) created a no-fault compensation program for vaccine-related injuries, shielding pharmaceutical companies from liability. This allowed vaccine manufacturers to continue using Thiomersal without addressing safety concerns.
The Fight for Answers: Cover-Ups and Denials
1998 - Wakefield and Mercury Concerns
Dr. Andrew Wakefield’s paper, though focusing on the MMR vaccine rather than Thiomersal, sparked widespread concern about vaccine safety. His claims catalyzed a public reevaluation of vaccine ingredients, including mercury-based preservatives.
1999 - Joint Statement and Removal Recommendations
After all the backlash to Dr. Wakefield, health authorities, including the CDC, FDA, American Academy of Pediatrics, and vaccine manufacturers issued a statement recommending the removal of Thiomersal from vaccines. This precautionary measure aimed to restore public confidence while maintaining vaccination rates.
2000 - The Simpsonwood Conference (or Fiasco)
A private meeting of CDC officials and scientists discussed early findings showing a 7.62x increased risk of autism linked to mercury exposure. Robert F. Kennedy Jr. wrote an article for Rolling Stone in 2005 titled “Deadly Immunity”, discussing the aftermath of this conference.
In June 2000, the Simpsonwood Conference, organized by the CDC, was held at a Methodist retreat in Norcross, Georgia. This meeting brought together 52 high-level officials from the CDC, FDA, World Health Organization, and major vaccine manufacturers such as GlaxoSmithKline, Merck, Wyeth, and Aventis Pasteur. The purpose was to review alarming findings about Thimerosal, a mercury-based vaccine preservative, and its potential link to autism and other neurological disorders.
Key Findings Discussed
Dr. Tom Verstraeten, a CDC epidemiologist, presented data from the Vaccine Safety Datalink (VSD) database. His analysis showed a 7.62x increased risk of autism in children exposed to Thimerosal-containing vaccines.
Additional studies highlighted a connection between Thimerosal and speech delays, attention-deficit disorder, and hyperactivity.
Despite these findings, attendees were more concerned about the potential legal and financial fallout than taking immediate steps to ensure public safety:
Dr. Robert Brent, a pediatrician, warned that the data could become a "resource to our very busy plaintiff attorneys."
Dr. John Clements from the WHO suggested that the study “should not have been done at all” to avoid misuse of the results.
According to RFK Jr. in his article, the conference participants spent much of the two-day meeting strategizing how to minimize public exposure to the findings rather than addressing the safety concerns.
The CDC withheld Verstraeten's original findings and delayed publication. When the study was eventually released in 2003, Verstraeten had reanalyzed the data under employment at GlaxoSmithKline.
Surprise, surprise.
He then significantly downplayed the link between Thimerosal and autism.
So, nothing came of Simpsonwood. Vaccine manufacturers continued selling Thimerosal-containing vaccines for years after the conference, even as they began phasing it out of U.S. markets. The surplus vaccines were exported to developing countries.
Another surprise: Autism rates subsequently began to rise in those countries.
“[The CDC] were giving us a guarantee, to be rest assured, there’s been no case of adverse effect [from the MMR vaccine] reported in any part of the world.”
“We had to compromise because we didn’t have any scientific proof that the administration of vaccines had any side effects.”
Peter Ayuk Enoh, Cameroon Delegate
The Simpsonwood transcripts, later obtained through Freedom of Information Act requests, fueled widespread criticism of the CDC and pharmaceutical companies for prioritizing industry profits over public health. The meeting remains a pivotal moment in the ongoing controversy surrounding vaccine safety and Thimerosal.
2004 - IOM Study and Continued Controversy
The Institute of Medicine (IOM) conducted a review of existing studies and concluded there was no evidence showing a “causal relationship” between Thiomersal and autism.
This is a similar argument to smoking doesn’t “cause” lung cancer.
The commentary that accompanied the study even said that “this study should put to rest parents’ concerns over the safety of the MMR vaccine.”
Put to rest: Aka, stop looking into this. Don’t do any more studies.
However, whistleblowers like Dr. William Thompson later alleged that the CDC had manipulated data to minimize associations between vaccines and adverse outcomes.
2002 - Legislative Protections
And it wasn’t just the medical community alone that was protecting the narrative surrounding Thimerosal. There were some heavy hitters:
George H.W. Bush - He was Vice President under Ronald Reagan from 1981-1989. The NCVIA was passed in 1986 during this time. He was President from 1991-1993. He was previously a board member of Eli Lilly.
George W. Bush - He was President from 2001-2009. His dad was George H.W. Bush. Enough said.
Mitch Daniels - George W. Bush’s former director of Management and Budget and a former Eli Lilly vice president.
Sidney Taurel - served on President George W. Bush’s homeland security advisory council. Was CEO of Eli Lilly while serving in the advisory council.
In 2002, a year after 9/11, President George W. Bush signed a the Homeland Security Act with a rider clause (written by Dick Armey, who later said the ‘White House’ told him to do it) protecting Eli Lilly, the manufacturer of Thiomersal, from lawsuits.

This amendment was repealed 2 months later, but the sneaky addition only showed how far the influence of Big Pharma stretched within the government.
Current State of Vaccines in Regards to Thiomersal
The Strawman - Anti-Thiomersal as “Anti-Vax”
Efforts to dismiss individuals raising concerns about Thiomersal as simply "anti-vaccine" have created a false narrative that obscures the real issues at hand. Many of these critics are not against vaccines; they are advocating for safer formulations and greater transparency about potential risks.
As Robert F. Kennedy Jr. stated in his 2005 article Deadly Immunity:
“We are not anti-vaccine; we are against toxic ingredients in vaccines that could harm children.”
By 2001, nearly all routine vaccines for children in the U.S. and Europe were Thiomersal-free. However, many vaccines were not “routine”, so they continued to contain Thiomersal in the multi-dose vials. Notably:
Seasonal Flu (25 micrograms of ethyl mercury per dose)
Adult Tetanus-Diphtheria (Td) (25 micrograms of ethyl mercury per dose).
Meningococcal (25 micrograms of ethyl mercury per dose).
Anthrax (varied amounts of ethyl mercury).
Smallpox (varied amounts of ethyl mercury).
Vaccines in 3rd World Countries
Thiomersal remains a critical component in vaccines used in many developing countries, primarily due to its role as a cost-effective preservative for multi-dose vials.
Multi-dose vials are significantly cheaper than single-dose alternatives. For example, the World Health Organization (WHO) estimates that the cost per dose for multi-dose vaccines is 30-50% lower than for single-dose vials.
According to the UNICEF Supply Division, over 60% of vaccines procured for global immunization programs still contain Thiomersal.
The World Health Organization (WHO) continues to endorse the safety of Thiomersal-containing vaccines, emphasizing their role in preventing millions of deaths annually. WHO maintains that there is no scientific evidence linking Thiomersal in vaccines to adverse health outcomes, including autism.
Coming Up: Do Vaccines Need a Rethink?
Are the recommended vaccines, as they stand today, truly essential—or could they be improved for a safer, more effective future? In the next part of our series, we’ll take on the big question: Are the recommended vaccines necessary?
LEARN MORE:
Learn more about the research behind the connection of Thimerosal to Autism in this documentary:

Informed Immunity: Are All Vaccines Necessary? (Part 3/3)

Vaccines are everywhere—from your baby’s first doctor visit to routine boosters as adults. They’re touted as life-savers, hailed as one of modern medicine’s biggest breakthroughs. But here’s the big question: Are all vaccines really necessary? Or are we taking shots in the dark, trusting a system that might need a second look?